What is Endodontics?
Endo” is the Greek word for “inside” and “odont” is Greek for “tooth.” Endodo 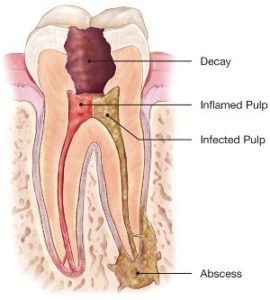 ntic treatment is treatment of the inside of the tooth.
ntic treatment is treatment of the inside of the tooth.
To understand endodontic treatment, it helps to know something about the anatomy of the tooth. Underneath the hard, translucent enamel and the less rigid, tubular structure called dentin, is soft-tissue called the pulp. The pulp contains blood vessels, nerves and connective tissue, from which both the dentin and the enamel are derived during early development.
The pulp spans the entire tooth, from the crown to the tip(apex) of the roots. Hence, inflammation, infection, and subsequent deterioration of the pulp can not only result in pain, but can also trigger breakdown of the surrounding bone and soft tissue (abscess), with which the pulp is in communication via an opening at the apex.
The most common reasons for inflammation or infection are deep cavities (caries), repeated dental procedures, cracks or fractures in a tooth.
Trauma, and even orthodontic movement (albeit very infrequently) can also cause inflammation and often shows up as discoloration of the tooth.
The remedy for these conditions is to remove the affected pulp. A fully mature tooth can survive without the pulp.
Endodontic Treatment
Endodontic Re-treatment
Apical Surgery "Apicoectomy"
Internal Bleaching


Pulp Cap "Pulpotomy"
Trauma Considerations


Re-evaluation